
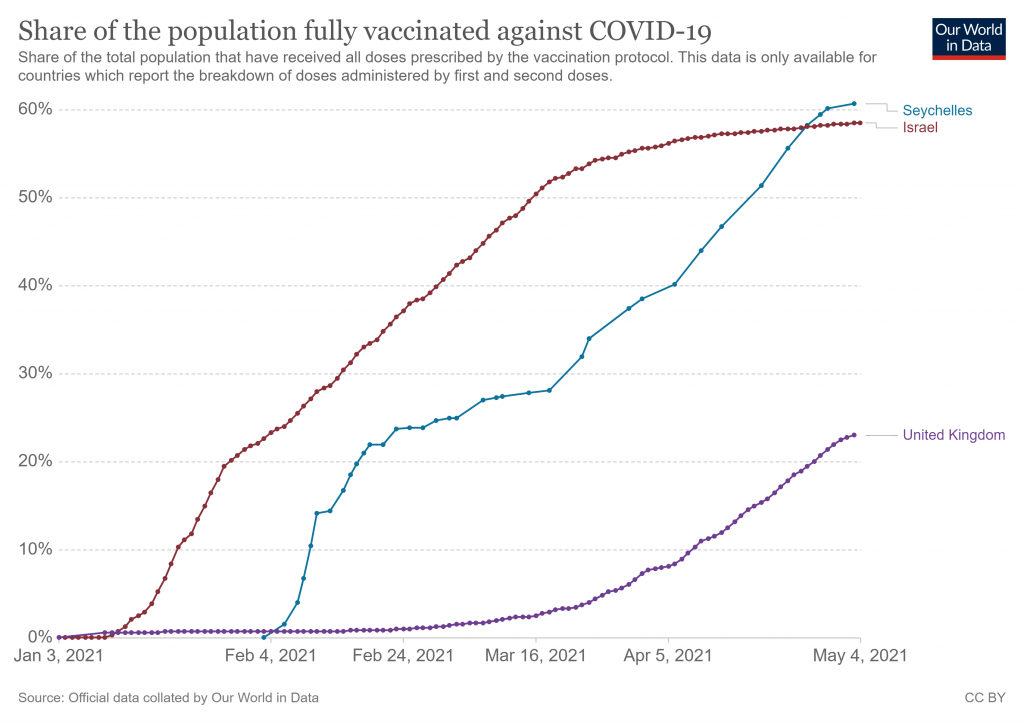
Seychelles, an archipelago nation in the Indian Ocean with a population of about 98,000, is locking down again – even though it has fully vaccinated more than 60% of its adult population with two vaccine doses, more than any other country in the world including Israel.
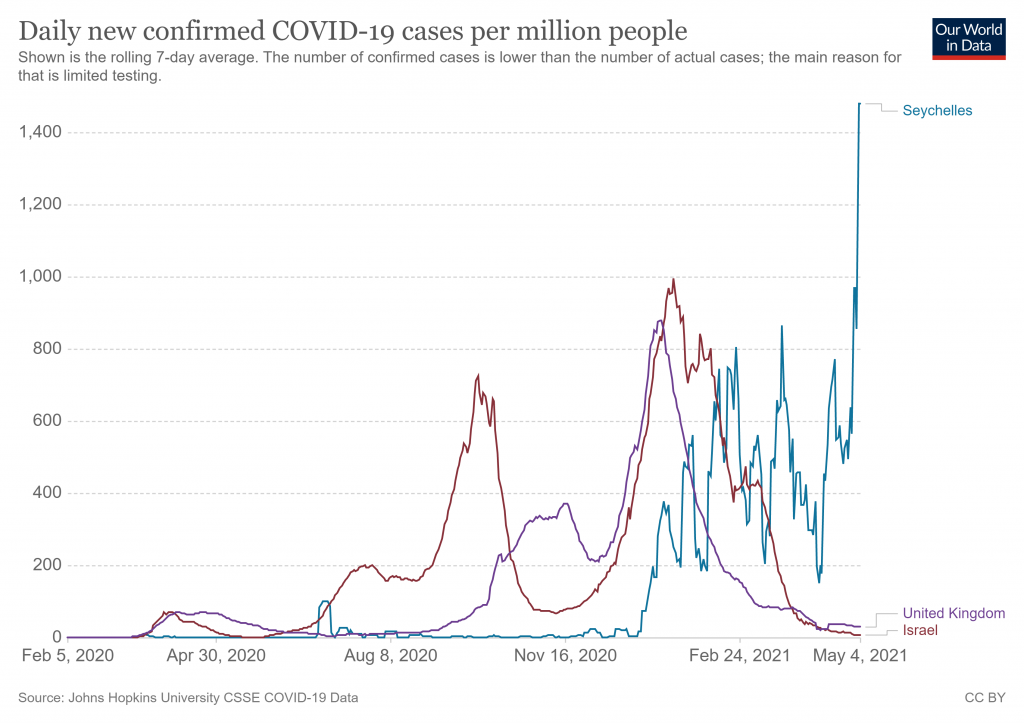
The country has banned the intermingling of households, closed schools, imposed curfews on bars and cancelled sporting activities for two weeks as infections surge.
The country began vaccinations in January using a donation of Chinese vaccines from the United Arab Emirates. According to Bloomberg, by April 12th, “59% of the doses administered were Sinopharm vaccines and the rest were Covishield, a version of AstraZeneca’s shot made under licence in India.”
The Government put the surge down to people being less careful, particularly over Easter. However, setting aside whether population behaviour is a plausible explanation, this doesn’t explain why the vaccines are not preventing transmission or infection.
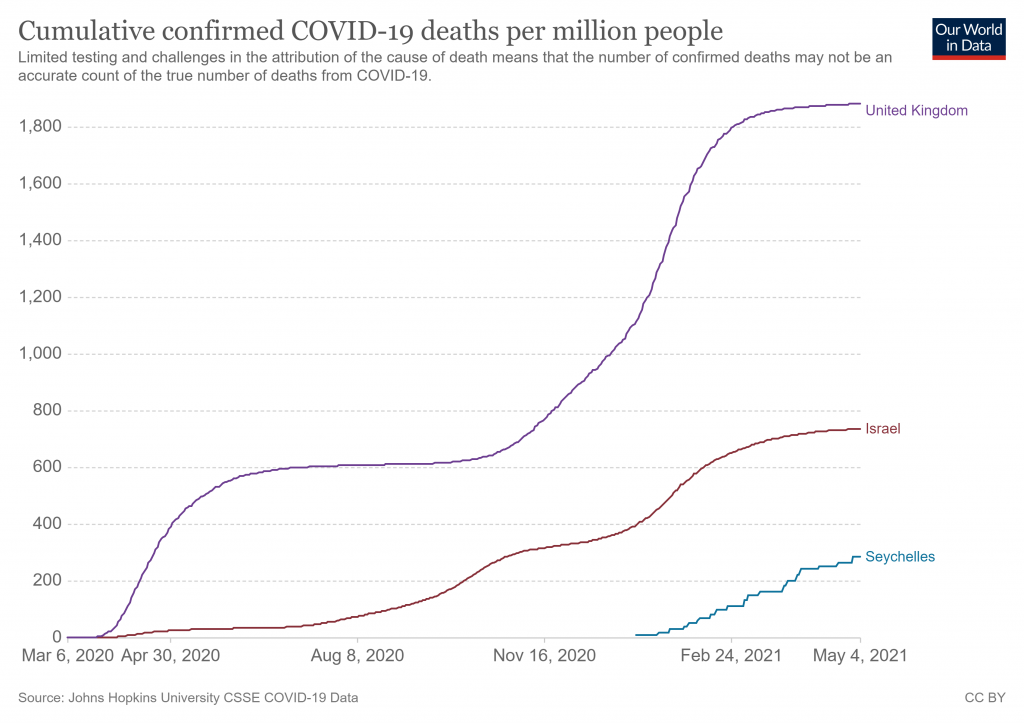
AstraZeneca and Sinopharm vaccines, particularly the latter, have not performed as well as Pfizer and Moderna vaccines in trials. Is this part of the explanation? Are they less effective in the vulnerable? Or perhaps they are better at preventing serious illness and death than mild or asymptomatic infection. Seychelles is still in its first wave, which only began at the end of December. Its deaths are still low and it will be interesting to see how they rise during this surge in positive cases. (There is no data available on testing numbers so we can’t see what role that might be playing.)
The late December epidemic began prior to the vaccination campaign starting in mid-January, but became worse during the roll out and has accelerated in the last week or so. Did the post-vaccine infection spike play a part? The fact that the country had not experienced a wave of COVID-19 before December means the acquired immunity levels are likely to have been lower than elsewhere.
A number of countries have low infection levels at the moment, including the UK and Israel with high vaccination rates, and Portugal (9% fully vaccinated) and South Africa (0.6%) with low vaccination rate.
The question is, if the vaccines don’t provide a way out, then why is the Seychelles locking down? The lockdown was originally supposed to “flatten the curve” until a vaccine came along. Once the population is vaccinated you might as well stop locking down because there’s nothing else to wait around in quarantine for. That a country that has fully vaccinated nearly two thirds of its population is locking down again as infections surge is ominous indeed.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Sinopharm in most actual tests looks to be very ineffective. (at most its 50%)
AstraZenica is also relatively poor at stopping infection at 65% and almost nothing against 484K variants (compared to mRNAs).
That ultimately means in reality only about 25% of their population has any protection.
This isn’t a massive surprise and could come back to bite us in the UK as well due to the majority AZ.
I wouldn’t describe 65% as relatively poor – unless it’s relative to Pfizer, perhaps.
Relatively to Pfizer/Moderna yes.
If AZ were our only vaccine it’d be fine but its not – there are far far better options.
It all stems from the government having a fairly irrational policy focussed on cases not sickness. With AZ people wont die but it wont have much of an effect on cases.
Its also pretty much impossible to hit herd immunity when 80% of people are vaccinated with something only providing maybe 65% protection.
“If AZ were our only vaccine it’d be fine but its not – there are far far better options.”
For the overwhelming majority of people, the best option is their own Mark I human immune system.
None of them are ‘vaccines’ , they don’t stop transmission or create immunity.
Before the WHO changed the definition, herd immunity is created when the majority of a population is exposed to the virus and creates antibodies and T-cells. That is still true.
Perhaps you have mispelled your ‘name’ a L rather than a R?
Relatively to Pfizer/Moderna yes.
They are all as bad as each other and none have addressed the inherent issue of ADE. The mRNA vaccines have additional toxicology problems. The adenovirus vaccines have their own unique potential problems as well. The Sinovac is most likely to have ADE problems.
The bottom line is you don’t vaccinate during an epidemic as you risk giving the virus or bacteria in question an evolutionary advantage. This is medicine and epidemiology 101, and as to which of the “vaccines” is “superior”, is entirely moot.
That’s the point – it’s an exaggerated relative risk reduction – a reduction fro a remote possibility
Indeed 95% in the approval to 65% now, when even at 95% the relative risk reduction was nothing to get excited about.
The number of people required to get vaccinated to prevent a single illness is growing rapidly.
Hundreds of people forced to take an experimental therapy to save a single person from getting ill. When the vaccines are creating illness quite readily, and death as well.
That relative risk reduction is looking pathetically positive right now.
Perhaps it is because the jabs turn people into spike protein factories and the single gene PCR processes run at 35+ cycle counts are designed to flag these as positive?
A perfect summary of the situation. I’m amazed that everyone keeps falling fur this wheeze!
The who said in Jan that only +ve test with symptoms can be counted. That’s why the numbers have been falling (after the massacre of the over 70s in January with the vax Logan’s run carousel)
Again – another example of the correlation with a rise following the introduction of vaccines.
Yes, another area where previously extremely low-level Asian-style outbreaks turned into European-style outbreaks or worse, once vaccination started 🙁
Could it be because the vaccines and tests are designed to work hand and hand to create a perpetual false pandemic to allow governments to implement draconian controls in perpetuity?
It’s more likely that they don’t make a difference at all with regard to transmissions and cases.
After the initial spike DUE to the ‘vaccines’ a country will have reached herd immunity due to this and prior infections, seasonal factored permitting/amplifying.
If prior infections weren’t sizeable enough though (Germany, Seychelles?!) the sh*tshow will just continue.
I think you may have hit on the truth.
Why, indeed! And ominous of what? Do you accept that vaccines do what they purport to do? What Is it they purport to do?
Why could be quite simple.
B.1.351 is the most dominant there (SA). We know AstraZenica (Covishield) is virtually useless against preventing infection against that.
Might just be they’re using by far the worst 2 vaccines available.
Clearly – even the government doesn’t believe that they do what they purport to do.
I asked here on Monday why when I left hospital, after an overnight stay, being told that I had to self isolate for ten days as one of my fellow patients had tested positive yet was telephoned the following day to be informed that ‘after further examination that patient was negative’ ?
I’m not an expert on cycles and wotnot but could they have used a lower cycle on testing him again ?
Someone replied that ‘perhaps they already had enough positives for that day’
or perhaps the thought of losing yet more staff to isolation was too much for management on a Bank Holiday.
Guidelines are clear that weak positives get retested (ideally on a fresh sample).
For safety reasons you assume that sample is positive until that’s been done.
No need for a conspiracy theory – its sensible guidance.
Thank you Splatt, as mentioned I’m no expert on the technicalities, didn’t even know there was such a thing as a ‘weak positive’.🙂
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/926410/Understanding_Cycle_Threshold__Ct__in_SARS-CoV-2_RT-PCR_.pdf
Page 7
Its also the WHO guidance ( https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05 )
Although PCR has issues (some quite big) there is a LOT of absolute nonsense spoken about it from people that have no idea of what it is or how it works.
This thread for example has several!
Name names! Or are you afraid?
Perhaps the inventor of the test can enlighten us. https://youtu.be/0zEoRmJgt00
Great news that you are free to go sit in the rain outside a pub again though.
Does “infections” mean +ve PCR tests? That is meaningless, and the reaction to it, as before, total hyperbole and this just shows that the hysteria is incurable by anything.
Or, are people falling seriously ill and being hospitalised? That would be much more serious and could lend support to the more negative assessment of the vaccines that have been postulated.
Because the politicians enjoy the power kick?
Lets face it – at the most basic level – the set of total prats that form the current cabinet (think no further than Hancock) could never gain significance in any other field.
I sound like a broken record, but here goes, again. The ABSOLUTE not relative results from the riculously small trials to date on the vaccines ( all of them) showed about 1% or less ability to provide immunity or stop transmission. All the bullshit media stuff after that and stupid ‘scientific’ analysis has just reflected the natural reduction in the virus in populations ( see Portugal for comparison).
What is reported increasingly is the effect of ‘spikes’ in blood vessel membranes from the vaccines themselves causing illness and deaths which when tested by the RT-PCR test will show as ‘covid19’.
Simply put, the politicians and scietists/medics pushing vaccinations are killing people, and the more booster vaccines etc , especially with the mRNA type will kill more. And the deaths will probably be delayed over time, maybe for years. As the immune system of the person involved may only violently react when they interact with a ‘wild’ coronavirus, probably any coronavirus like the ones that constitute 25% or so of the ‘common cold’.
This issue has gone beyond lockdowns, its now entered the dystopian world of mass murder.
Not really. You can only provide a relative risk figure after a short period but that does not mean the absolute risk is only ~1%. That can only be true if there are no further infections. The added problem is that the trial was being carried out when viral prevalence was low so the numbers were always likely to be small.
In truth, we don’t really know what the Absolute Risk (AR) is. If the pandemic was just starting in a 100% susceptible population then AR = RR. That’s clearly not the case so AR will be lower – perhaps quite a bit lower given the timing of the vaccine rollout. I’d guess about 0.3 x RR in Dec/Jan
That is gibberish. The trial results show what they show. Absolute reductions of about 1%. All you are saying, without admitting it, is that hardly anyone got the disease. Well that is true, hardly anyone gets it. So you inject all the population for something about 1% gets and of them about 0.15% die.
Yes its stupid. But criminal is knowing that of the 100% population you aim to inject a sizeable proportion stand a real risk of death from the injection.
The problem is that “they” know the absolute numbers are the only wants that count, and deliberately quote absolute numbers whenever it suits their agenda. It gets worse though: Not everyone can catch COVID-19; Many have pre-existing immunity so would never be a viable ‘host’; Studies show this is about 50% of the population. https://www.hartgroup.org/mortality-data-covid-19/ I’ve also seen studies that suggest upwards of 80% of the population are immune. The bottom line is that the “vaccines”are a net negative to the vast majority of the population. Perhaps, all the population. Arguing about relative and absolute is important, but it’s ignoring the 400 pound gorilla in the room – Antibody Dependent Enhancement. I have been trying to find out how soon this phenomena can kick in. I watched a video with Sucharit Bhakdi last night, and he said “immediately”. So the question is this: in almost every country in the world, we see a sharp rise in Covid cases and deaths, with Seychelles being a prime example. What is causing this? Could it be ADE? Could it be vaccine deaths caused by the “vaccines” themselves? Could it actually be Covid deaths because of the drop in natural immunity for a few days?… Read more »
It is not “gibberish”. Mayo has provided a clear explanation of the utility of the relative risk reduction metric, where it is impractical to make observations for an extended period.
Whether the study design, and the actual data collected, reasonably permit the quoted result to be taken as meaningful, is a separate matter. Clearly, very few significant outcomes were observed in either group, and confounding factors may well have been insufficiently addressed.
Had the study been conducted over a longer period, or, indeed, had SARS-CoV-2 been of greater prevalence, during the study, there would, surely, have been a greater number of significant outcomes, in each group. Thus, it would have yielded a larger absolute risk reduction. However, on the assumption that the actual, and hypothetical, results are robust, the relative risk reduction would be the same.
Had the trials actually included more old people, and not fit and healthy volunteers, there would have been way more deaths and the trials would (hopefully) have been abandoned.
Why did they skip animal trials and go straight to humans?
I agree we are arguing over exceedingly small sample sizes, but that makes the situation even worse.
This is the most unethical, morally bankrupt experiment I have ever seen (outside of Mengele and things the US and Israel have done, of course).
I fear you have misunderstood me.
When I posted about “the utility of the relative risk reduction metric”, I was referring to the metric as a concept, not to the specific result obtain in a particular “vaccination” study.
I made absolutely no endorsement of any study.
And, for those who down-voted: Is any of you capable of explaining any error in what I wrote, or were you just participants in one of those infinite monkeys experiments?
Plenty of people get the disease. I’m nearly 70 and this is the most wide spread disease I’ve ever witnessed. Fit young guys who I know well (sons and nephews) have been laid up for 2 weeks and more. My daughter’s partner is a regular Iron Man competitor. Even 3 weeks after his symptoms first appeared he was having coughing fits which caused him to throw up.
But don’t take my word for it. Listen to what the doctors recommending Ivermectin and/or Hydroxychloroquine say about Covid. Pierre Kory is adamant that Covid is not “just the flu”. It causes a very unpleasant relatively long lasting illness.
But back to the main point. The Pfizer data was being collected in the summer when virus prevalence was low.
The bottom line is that you can’t calculate the Absolute Risk of a respiratory virus from a short time period – particularly if the virus is seasonal.
“I’m nearly 70 and this is the most wide spread disease I’ve ever witnessed. “
Well – you must have done a Rip van Winkle for nigh on 70 years! – because every year prior to 2003 reaped a bigger harvest of mortality – the real acid test of respiratory disease severity.
No-one is saying that a bad dose isn’t very unpleasant (and dangerous in the vulnerable) – just like ‘flu – but it isn’t exceptional in either short or longer terms. Being laid up for two weeks – or longer – is common with a bad dose of real ‘flu (as opposed to a bad cold), and in terms of contrary subjective experience, I’ve known only one person who had it really badly. I had a bug in 2019 which induced severe coughing for 3 weeks or more.
Its exceptionality is in the political, not the physical sphere.
The hysteria about this moderately severe virus is the main sickness. And clearly, the ‘vaccines’ are highly questionable both in terms of benefits and harms.
… and low levels of risk reduction.
“that does not mean the absolute risk is only ~1%. That can only be true if there are no further infections.”
No. It’s a sampled proportion of instances over a specified time period – the same as relative risk. It’s a measure of actual rather than the deceptive comparative reduction in risk – i.e an indicator of real risk reduction.
In truth, we don’t really know what the Absolute Risk (AR) is.
… and that is pure nonsense. As with RR we know it in terms of the usual benchmark of probabilities gleaned from a sample.
Sorry to piss on your vaccine pansies of figures for the gullible. You suckers do want to believe sooo badly!
You might find this interesting if you havnt already seen it.
https://blogs.bmj.com/bmj/2021/01/04/peter-doshi-pfizer-and-modernas-95-effective-vaccines-we-need-more-details-and-the-raw-data/
The “95% efficacy” is cobblers.
I’m sure you know how they calculated it in the trials.
1-(8/162)x 100 = 95%
However they left out ~3500 people with “suspected COVID” but which didn’t have a positive PCR test.
So throughout this year the “experts” and media have used the line that the “False negative” Rate is so high that there are more “concerned” with missing possible infections (ie a false negative) So they accept the false positives.
Yet here they just ignore the extra 3500 suspected CV cases which would reduce the efficacy to 19% at best.
Prof Bhakdi has a good take on the “95%” calculation:
Perspectives on the Pandemic | “Blood Clots and Beyond” | Episode 15 – YouTube
Bloody snake oil doesn’t work, does it?
Spi-M-O (Sage advisory) doesn’t think so: 32. The resurgence in both hospitalisations and deaths is dominated by those that have received two doses of the vaccine, comprising around 60% and 70% of the wave respectively. This can be attributed to the high levels of uptake in the most at-risk age groups, such that immunisation failures account for more serious illness than unvaccinated individuals. This is discussed further in paragraphs 55 and 56.Who becomes seriously ill in a resurgence? 55. Figure 11 illustrates the age and vaccination status of those hospitalised (left) and dying (right) over time in Warwick’s central sceenario for the whole Roadmap (equivalent to Figure 4). The top plots are absolute numbers and the bottom plots are as a proportion of those admitted or dying.This shows that most deaths and admissions in a post-Roadmap resurgence are in people who have received two vaccine doses, even without vaccine protection waning or a variant emerging that escapes vaccines. This is because vaccine uptake has been so high in the oldest age groups (modelled here at 95% in the over 50-year olds). There are therefore 5% of over 50-year olds who have not been vaccinated, and 95% x 10% = 9.5%… Read more »
I think we should constantly point out that even the government obviously doesn’t believe in the ‘vaccines’ on which they spent shed loads of public money and are desperately trying to avoid the obvious conclusions.
Iain Davis has produced another cracker over at UKcolumn.
If you wondered who was behind the global consistency of messaging about SARS2/covid, read about Omnicom and OmniGOV.
https://www.ukcolumn.org/article/buying-a-single-version-of-the-truth
“Providing a “single version of the truth”
Omnicom was awarded the contract on 21st May 2018. On the 9th June (less than 3 weeks later), then UK Prime Minister Theresa May announced that the G7 had agreed to her Rapid Response Mechanism. Canada, France, Germany, Italy, Japan, the UK, the US and the EU agreed that they would assert a common narrative.”
Something in there about organ donation too, supporting the NHS “their hands on your glands” marketing propaganda. I refuse to register ever again, since the principle of “presumed consent” was introduced. Consent cannot ever be presumed, it makes a mockery of it.
Mate, hate to say this but UK Column might have been pulled by their domain registrar or hosting company:
https://www.ukcolumn.org/
This site can’t be reachedThe webpage at https://www.ukcolumn.org/ might be temporarily down or it may have moved permanently to a new web address.ERR_NAME_RESOLUTION_FAILED
No just a temporary problem, it’s back.
Alex Belfied is back on YouTube after being banned for a week and asks a pertinent question.
Why has British Airways just cancelled his 30th May flight to America when we are supposed to be able to be able to fly abroad from the 17th ?
(And also put flight crew on furlough until June).
A bit daft as the US still has a ban on UK/Schengen travellers for entry other than a few stated exceptions. I have pointed out its not too difficult side-stepping this, but not by booking a direct flight with BA.
Does him being a journalist count as a stated exception ?
“Major Study Finds “Abundance of Patients Admitted to Hospital With Covid Within Seven Days of Vaccination””
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/982499/S1208_CO-CIN_report_on_impact_of_vaccination_Apr_21.pdf
They are still trying very hard to maintain the notion that the vaccinated people suddenly got infected just as they had the vaccination or shortly afterwards; ie its all their fault for being stupid. Although the other categories they label with less certainty ( ie they are very certain that people are stupid) show alarming trends.
They have worked hard to put out a seemingly informative report with many caveats and one big assumption, people are thick.
Looks more likely that the jabs caused ill health of some kind perhaps even COVID symptoms.
“Major Study Finds “Abundance of Patients Admitted to Hospital With Covid Within Seven Days of Vaccination”” Holy mackerel Steve, great find! Summary This report investigates hospitalised vaccinated patients during the second wave of the UK COVID19 outbreak using the ISARIC4C / CO-CIN data set with data available up to April 10th 2021. For patients enrolled to ISARIC4C / CO-CIN: • 1 in 14 patients admitted to hospital since December 8th 2020 have received at least the first dose of a COVID-19 vaccination (previously 1 in 25). • The median time between vaccination and symptom onset for these patients was 9 days. • The median time between vaccination and hospital admission for these patients was 15 days. • Most vaccinated hospitalised patients were infected shortly before or around the time of vaccination, and others after vaccination but before immunity had developed (immunisation) [high confidence] • As the period of follow-up observation has increased, there has been a rise in the proportion of SARS-CoV-2 PCR positive people admitted more than 21 days after vaccination (vaccine failure) [moderate confidence]. However, while absolute counts are low and continue to fall as the risk of exposure continues to fall, this will lead to under-representation the… Read more »
because lockdowns have nothing to do with vaccines…. obviously
If vaccines are ineffective but carry risks you are exposing people to covid risk + vaccine risk… get your head round that one covidians.
I noticed that gets often overlooked – its not a binary choice. For some it will be increased risk because the risk will be vaccination risk plus covid risk as you state.
And, those who have already had Covid, are exposed only to the vaccine risk.
A picture says a thousand words.
This is the chart LDS seems unable to publish to explain What is going on in Seychelles.
For more like this go see this
https://mobile.twitter.com/MConceptions
Almost every country can pinpoint its “spike” with a well known roll out of V day
D-Day more like. If D stands for Death.
Do the Seychelles have a Covid passport app yet?
Surely the vaccines only work once accompanied by the app? Or something
https://mobile.twitter.com/JordanSchachtel/status/1390015401673777153
Did you know almost 4,000 children have been vaccinated for COVID-19 in the States?
And that:
9 died within 28 days (0.2%)?
7 almost died?
3 were permanently disabled?
71 had to see a doctor or were admitted to hospital or had their stay prolonged?
Why isn’t this headline news?
So these children died or were maimed (possibly for life) for a virus that all children are almost completely immune to. Pointless, heart breaking and totally unnecessary deaths. What possessed their parents to allow this to happen in the first place? What on earth possessed the medical teams who went along with it? (First, do no harm…) And what will happen to the children who have not yet had an adverse reaction to the experimental jab? Disability or death a few years down the line? Infertility? It appals me that they have extended this to children who have no choice in the matter. It is too evil for words. And the complicity of MSM with the current narrative have made them nothing short of accessories to murder. I look forward to a day of reckoning.
Without knowledge of the testing rate and its accuracy, the “infection” rates are meaningless.
Deaths are still low.
In the UK Government and mainstream media promoted Coronavirus mortality numbers are of those who have died within 28 days of a positive Coronavirus test result IRRESPECTIVE OF THE ULTIMATE CAUSE OF DEATH or with ‘Covid19 or Coronavirus mentioned on the Death Certificate irrespective of the context of the mention.
Please confirm by referring to FOI’s submitted via What do they Know to the UK Office of National Statistics or to Public Health England.
I have serious concerns about the Sinopharm vaccine. It’s a traditional inactivated whole virion vaccine and they tend to give a poor response in the elderly. Also if the majority of the young population aren’t vaccinated then it’s easy to see how the virus could spread rapidly among them if it got a hold; the important thing to watch is the severity of the infection in the elderly. If the vaccine is preventing serious disease in the elderly an outbreak in the young healthy population isn’t too much concern.
Gibraltar claim to have a totally vaccinated population. Will be interesting to see how that goes as they are reported to have open borders without conditions.